Overcoming Vaccine Hesitancy: Meeting People Where They Are
In India, deeply ingrained cultural beliefs about sexuality and gender roles contribute to vaccine hesitancy. These norms may give rise to concerns about side effects or moral implications of the HPV vaccine.



A village in the remote hills of Nepal. The sun is setting, and the local radio station is on. A catchy tune begins playing, followed by lyrics that sound like a playful debate between two people. But these lyrics are not just for entertainment - they're about COVID-19 and vaccines, and they're meant to build trust and dispel rumours in the community. The "Khelo Dohori" radio series, which translates to "Playful Debate" in English, is part of a public health initiative in Nepal. The series employs a culturally relevant approach to address the pressing issue of vaccine hesitancy among local communities. Such hesitation toward vaccines is a global concern, and it is particularly prevalent in developing countries.
Shifting our focus to India, cervical cancer is the second leading cause of cancer-related deaths among Indian women, yet only 1% of the girls are vaccinated and less than 2% are screened. India's share in global cases is a staggering 21 per cent in cervical cancer. This is due in part to the high cost of foreign vaccines. In response, India has introduced Cervavac, a cost-effective, domestically developed Human papillomavirus (HPV) vaccine. It is poised to become part of the national immunisation program, initially targeting girls aged 9 to 14. However, providing the vaccine is just the first step, as familiar patterns of vaccine hesitancy persist, largely rooted in beliefs and limited knowledge about immunisation.
To understand vaccine hesitancy, including for the HPV vaccine, we need to consider the mental models that shape people's attitudes and behaviours. These mental models are shaped by a range of factors, such as socioeconomic status, gender, geography, religious and cultural beliefs, and personal experiences. These factors interact with people's access to information about vaccines, leading to diverse mental models and diverse vaccine attitudes and behaviours. In India, deeply ingrained cultural beliefs about sexuality and gender roles contribute to vaccine hesitancy. These norms may give rise to concerns about side effects or moral implications of the HPV vaccine. Together, these factors can create a complex web of barriers to vaccination.

In India, for example, deeply ingrained cultural beliefs about sexuality and gender roles contribute to vaccine hesitancy. These norms may give rise to concerns about side effects or moral implications of the HPV vaccine. For example, some people may believe that the HPV vaccine is only for sexually active women, or that it encourages promiscuity. The sexual education gap and cultural factors at play contribute to resistance to the vaccine among both family members and healthcare providers, leading to lower uptake and increased risk of cervical cancer. These beliefs can be powerful barriers to vaccination.
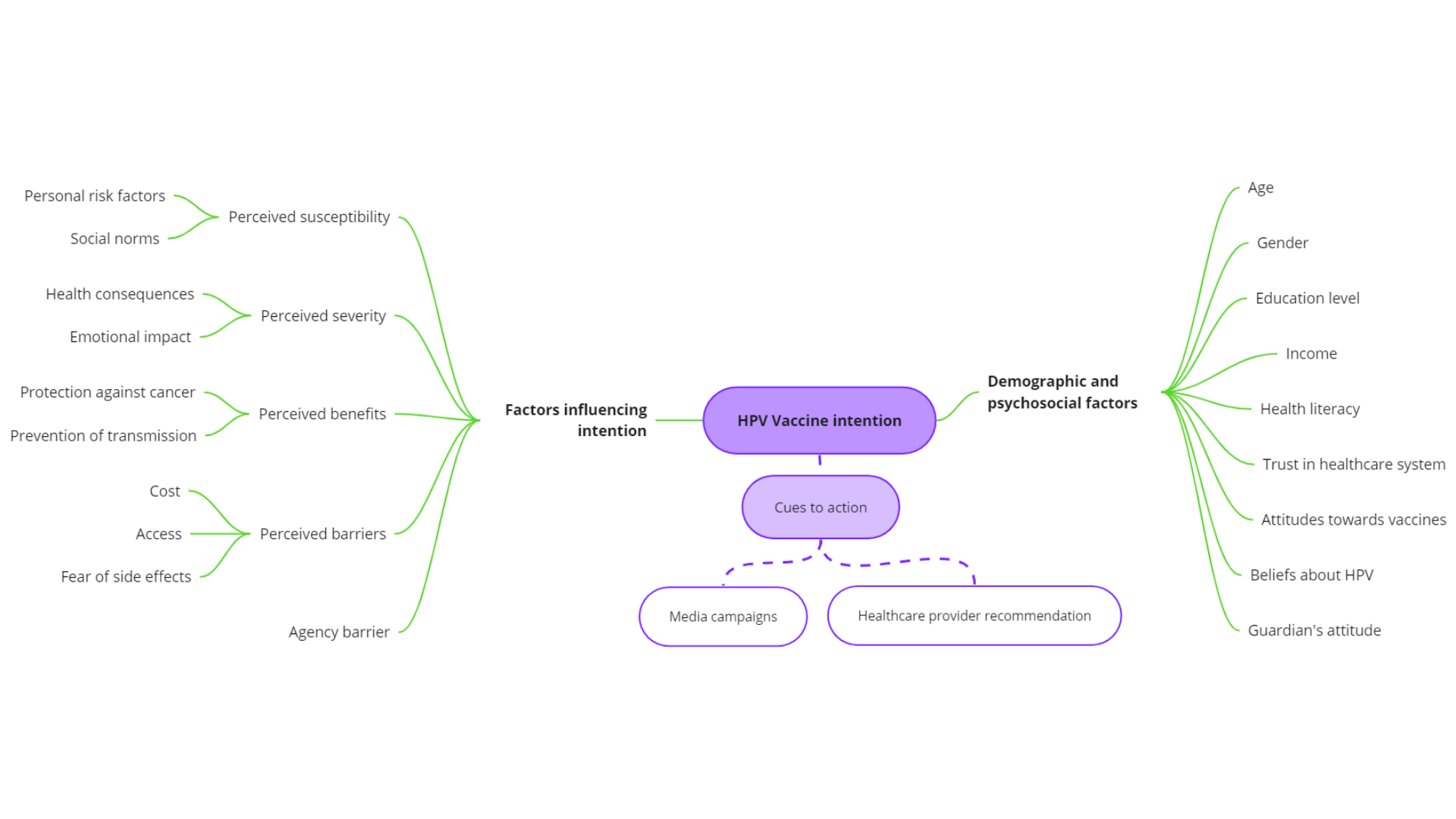
Below is a mental model based on existing literature(Kataria et al., 2022; You et al., 2020; Paul et al., 2013) to understand the factors that play a role in vaccine hesitancy of the HPV vaccine.
Vaccine decision-making can also be influenced by cognitive biases such as the 'peanut effect' and confirmation bias. The 'peanut effect', a tendency to overestimate rare events while underestimating common ones, may impact perceptions of vaccine risks(Weber & Chapman, 2005). For example, some individuals wrongly believe that HPV vaccines could lead to risky sexual behaviour despite the lack of evidence supporting this claim. This misbelief leads them to focus disproportionately on potential side effects rather than recognising the much higher risk posed by HPV infection itself. Such biased approaches towards risk assessment hinder effective decision-making, with implications for public health outcomes.
Are some communities more vaccine-hesitant than others?
Research indicates that vaccine hesitancy is influenced by a variety of factors, including socioeconomic status, educational level, religious affiliation, and location. Migrant backgrounds, and minority groups tend to have lower trust in institutions and are thus more likely to be hesitant about vaccines. Additionally, people in remote areas face unique challenges in accessing vaccines, which can further exacerbate vaccine hesitancy(Wong et al., 2020; Dhalaria et al., 2022).
Can we customise? Tailoring health messaging

In response to the COVID-19 pandemic, innovative methods have arisen to address vaccine hesitancy. These initiatives encompass various forms of media, such as the Local Champion’s video series in India, the "Khelo Dohori" radio series in Nepal, the Cootie shot song in the US, and TikTok videos that creatively incorporate popular lyrics to promote vaccination and dispel misinformation. These creative approaches proved successful by leveraging trust within local communities and cultural traditions. Trust plays a pivotal role in motivating individuals to make informed decisions, including opting for vaccination. By integrating principles from behavioural science with culturally relevant strategies, the radio series has effectively transformed people's knowledge, attitudes, and behaviours concerning vaccines. Moreover, it is crucial to address ideological factors contributing to vaccine hesitancy when devising comprehensive strategies.
As the immortal words of Mary Poppins remind us, sometimes we need "a spoonful of sugar to help the medicine go down." However, when it comes to addressing vaccine hesitancy, we can't simply rely on a universal "spoonful of sugar." We need to carefully consider the specific factors influencing vaccine uptake in different communities.
See you next week!
Before I go, I would like to leave you with a catchy COVID-19 vaccination song that has been stuck in my head as I write this:



